Thailand's first cannabis clinic opened on Monday (Jan 6) and was flooded with patients after the country became the first in Asia to legalise medicinal use of the drug.
Hundreds of patients converged on the government run facility in Bangkok - which already has a waiting list of more than 2,000.
The pilot clinic, based in the Ministry of Public Health, expects to see between 200 to 300 patients daily.
Public Health Minister Anutin Charnvirankul said today that patients would receive free treatment for the first two weeks. He said: ''This is a pilot clinic, because we cannot produce enough doctors with expertise in cannabis.''
The Southeast Asian country legalised marijuana for medical use and research in 2017. While in 2019 it removed cannabis and hemp extracts from its banned drugs list and pushed laws allowing each household to grow up to six plants.
In a protectionist move to boost the country's economy, only domestic drugs firms and farmers will be able to supply the country's network of clinics.
Health Minister Anutin Charnvirankul said there were already around two dozen smaller non-specialist cannabis centres that form part of general hospitals that see patients sporadically.
But the clinic he opened today (Jan 6) is the first one that will be the first full-time facility staffed by doctors who are experts in medicinal marijuana, he said.
Thailand plans to open 77 similar clinics in the future - one in each of its provinces.
Source: https://www.newsflare.com/video/331975/other/thailands-first-cannabis-clinic-opens-in-bangkok
Israeli researchers have developed a medical protocol detailing how cannabis in the elderly should be best treated, and also examined in a preliminary study. The results are impressive - 85% reported an improvement in their health, and researchers recommend that doctors consider the treatment of elderly cannabis as an alternative to narcotic drugs.
Shay Friedman
Cannabis treatment is effective for elderly people with chronic pain, sleep deprivation, loss of appetite, nausea, and post-traumatic stress disorder (PTSD), helping to reduce their use of narcotic drugs In the elderly with cannabis in the best way.
Researchers at Ben Gurion University, Soroka Hospital's Cannabis Clinical Research Institute, and Niamedic Clinic conducted a study designed to test the efficacy of the medical protocol they developed, which involved 184 elderly patients treated with cannabis according to the protocol and monitored for six months.
The results of the study, together with the therapeutic protocol itself, were published last month in the Journal of Clinical Medicine, entitled "Medical Cannabis for Older Patients - Protocol of Treatment and Preliminary Results". The research was carried out by Dr. Ran Abuchatzira, Dr. Adi Ron and Inbal Sikorin.
Medical Cannabis for the Elderly - Treatment Protocol
"Because there are no established protocols with proven efficacy in treating elderly people with medical cannabis, we have developed one of ours that emphasizes close examination of the effects and side effects, and a slow and gradual start of THC oil, CBD oil, or a combination of the two [and not smoking]," says D. ”Dr. Abuhtsira of the Faculty of Medical Sciences at Ben-Gurion University.
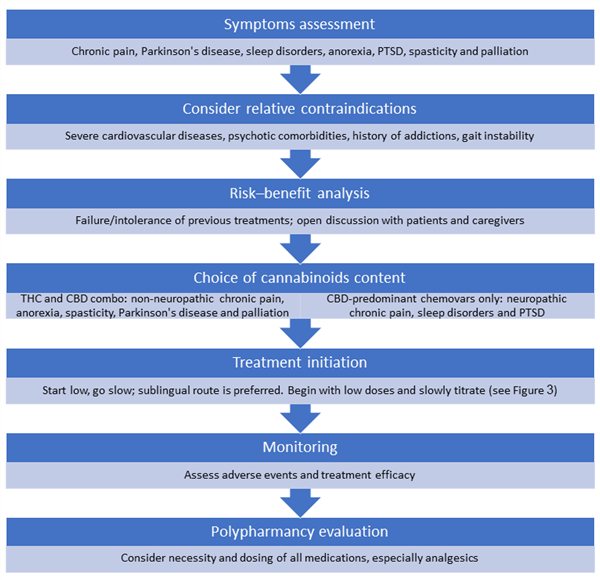
According to the protocol, there are two cornerstones on which the treatment of cannabis in the elderly should be based: starting the lowest dose and gradual increase, and frequent monitoring and review. The goal is to reduce the side effects of treatment as much as possible, with the key phrase for researchers being 'non-harmony primacy' ('first, do no harm') - a fundamental principle of medical ethics.
The first steps, therefore, are designed to ensure that cannabis treatment is indeed appropriate for the patient. The appropriate contraindications for treating elderly cannabis by protocol are chronic pain, Parkinson's disease, sleep disorders, post-traumatic anorexia, convulsions, and palliation (alleviating the suffering of terminally ill patients). Severe cardiovascular disease, risk factors for psychosis, history of addictions, and problems with posture are the contraindications that the physician should consider as reasons to avoid cannabis treatment.
The treatment protocol also places special emphasis on the issue of polypharmacy (multi-drug) in the elderly, with the end goal being that successful cannabis treatment will allow the geriatric patient to reduce the doses of the other drugs he is taking, and even stop taking them. This is actually the last step in the treatment protocol, as seen in the diagram:
“If the treatment is effective and the side effects are not severe, a change in the concomitant treatment with other drugs, especially discontinuation or dosing of opioids, benzodiazepines, and psychotropic and other analgesics, can be considered. Our experience shows that cannabis has the potential to reduce the use of these drugs, ”said Dr. Abuhtsira.
The protocol also addresses concerns that may arise in older patients about the use of cannabis: "The stigma associated with the use of 'cannabis' may prevent patients from agreeing to medical cannabis treatment - even though it is a relatively safe and effective drug," it said. “It is therefore very important to explain to the patient and his / her family the potential benefits and dangers before starting cannabis treatment. This explanation should be given by a nurse or doctor who is proficient in cannabis treatment. ”
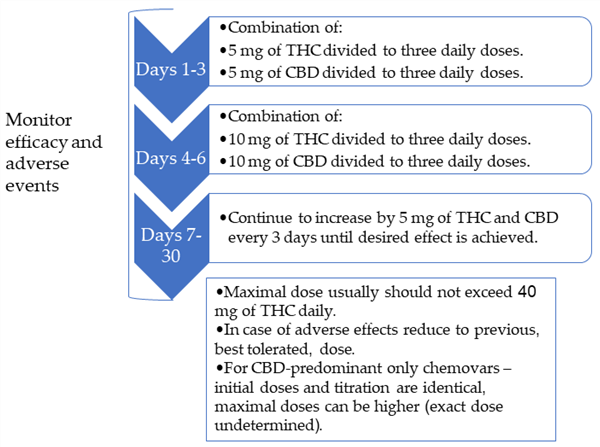
Cannabis dose I started to treat the elderly: 5 mg / day
The next step is to determine the cannabinoid ratio and the appropriate dose for the patient. The recommended method of consumption, according to the protocol, is always a sub-lingual drizzle of cannabis oil. For most labels, researchers recommend oil with an equal ratio of THC to CBD ('balanced'), or a combination of dominant THC oil with dominant CBD oil, so that an equal dose of both is obtained.
For the labels of chronic pain from neuropathic origin, sleep disorders and post-traumatic stress, it is recommended to treat only CBD-containing oil with as little as THC.
The recommended starting dose is 5 mg of THC and CBD (or only CBD, depending on the schedule) per day, divided into three daily doses - 1.7 mg per dose. This is exactly the dose that contains every drop of cannabis oil with a concentration of 5% THC and 5% CBD, so it is the ideal concentration for starting treatment.
The dose should be increased by 5 mg every 3 days, until an effective dose is reached. In case of side effects, you should reduce back to the previous dose for another 3 days, then try raising again.
The maximum daily dose recommended in the protocol is up to 40 mg THC per day. For those who are treated with CBD alone, they do not have a maximum dose of 40 mg, but CBD therapy is recommended to start with the same dose and gradually in combination with THC and CBD.
Elderly care for cannabis: 85% satisfied
184 patients with an average age of 81.2 participated in the study through a customized geriatric clinic. After 6 months of cannabis use 58.1% of them chose to continue cannabis treatment and the rest discontinued for such and other reasons, which probably shows that treatment is not suitable for everyone.
Of those who continued treatment, 84.8% reported that there was a moderate or significant improvement in their health status from the start of treatment, and 44% reported that there was a significant improvement in their health status since the start of treatment.
33.6% of patients reported any side effects, with the most common being dizziness (12.1% of patients) and fatigue / fatigue (11.2% of patients). It is important to remember that this is an adult population that is sensitive to side effects, and according to the researchers "the rate of side effects, especially the serious side effects, was relatively low".

Source: https://in.bgu.ac.il/en/pages/news/cannabis_geriatric.aspx
Source: https://www.mdpi.com/journal/jcm

Effects of Cannabinoids on Female Sexual Function
Becky Lynn, MD,1 Amy Gee, MD,1 Luna Zhang, BS,1 and James G. Pfaus, PhD2
ABSTRACT
Introduction: With the legalization of both medical and recreational marijuana in some countries and a few US states, its use has become more widely prevalent. Both exogenous cannabinoids such as tetrahydrocannabinol (THC) and endogenous cannabinoids (endocannabinoids) have been shown to affect female gonadotropin pathways and female sexuality. Yet, our understanding of the mechanisms and effects on female sexual function is limited.
Aim: To review the literature regarding the effects of both endogenous and exogenous cannabinoids on female sexual function in both animals and humans.
Methods: We performed a PubMed search for English-language articles in peer-reviewed journals between 1970 and 2019. We used the following search terms: “cannabinoids,” “endocannabinoids,” “marijuana,” “cannabis,” and “female sexual function” or “sexual function.” The main outcomes of the papers were reviewed.
Main Outcome Measure: The main outcome measure was sexual function in females.
Results: A total of 12 human studies and 8 animal studies that evaluated the relationship between cannabinoids and female sexual function were included. Study types in animals were blinded, prospective, placebo-controlled trials. Human studies were based primarily on questionnaire data. The data indicate dose-dependent effects on female sexual desire and receptivity, such that low doses generally facilitate or have no effect but high doses inhibit.
Conclusions: More research is needed to develop a better understanding of the effects of cannabinoids on female sexual function. There does appear to be an effect on both animals and humans, but whether the effect is positive or negative along dose and species lines requires more study. With the legalization of marijuana occurring in more countries and more US states, there needs to be more well-controlled studies evaluating the effects. Lynn B, Gee A, Zhang L, et al. Effects of Cannabinoids on Female Sexual Function. J Sex Med 2019; XX:XXXeXXX.
Copyright 2019, The Authors. Published by Elsevier Inc. on behalf of the International Society for Sexual Medicine.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Key Words: Endocannabinoids; Cannabis; Marijuana; Female Sexual Function; THC; Endocannabinoid System
INTRODUCTION
Marijuana use has become more widely prevalent over the last decade. Its use has been decriminalized in México and has been accepted into law for both medical and recreational purposes in
Received May 9, 2019. Accepted July 22, 2019.
1Department of Obstetrics, Gynecology and Women’s Health, Division of General Obstetrics and Gynecology, Saint Louis University School of Medicine, St. Louis, MO, USA;
2Centro de Investigaciones Cerebrales, Universidad Veracruzana, Xalapa, Veracruz, México
Copyright ª 2019, The Authors. Published by Elsevier Inc. on behalf of
the International Society for Sexual Medicine. This is an open access
article under the CC BY-NC-ND license (http://creativecommons.org/
Canada and for use by the general population in several US states. As of the publication of this paper, 33 states and the District of Columbia had legalized marijuana for medical use, and 10 of those states legalized marijuana for recreational use.1 Good-quality research has long been lacking on the effects of marijuana on sexual function due to the illegality of the drug. The effects of marijuana on physiological mechanisms and be-haviors that drive sexual function have been studied primarily in rodents, and human research has had to depend on retrospective questionnaires. This paper aims to review the published data assessing the effects of cannabinoids on female sexual function.
METHODS
A literature review was performed in PubMed for publications in English with the keywords “marijuana,” “cannabis,”
“endocannabinoids,” and “sexual function” or “female sexual function.” We found 190 articles with these search qualifications, and the abstracts of these 190 articles were reviewed. Articles were included if they featured a study or survey that measured the impact of marijuana usage on female sexual function in an-imals and/or humans. Citations in these articles were then also reviewed for relevance. Given the scarcity of research done on humans relating to marijuana usage and sexual function, any relevant article was selected. No particular type of study was excluded or sought out. Twelve articles were identified relating to human research and were reviewed; of these 12 articles, 11 were retrospective surveys, and 1 was a prospective cohort study. Eight prospective, randomized, blinded animal studies were included. No particular animal species was included or excluded, but the animal studies relevant to this review were largely done on rats. Our main outcome measure was sexual function in females.
Endocannabinoid System
The first biologically active component of cannabis was identified in the 1960s as D9- tetrahydrocannabinol (THC), a
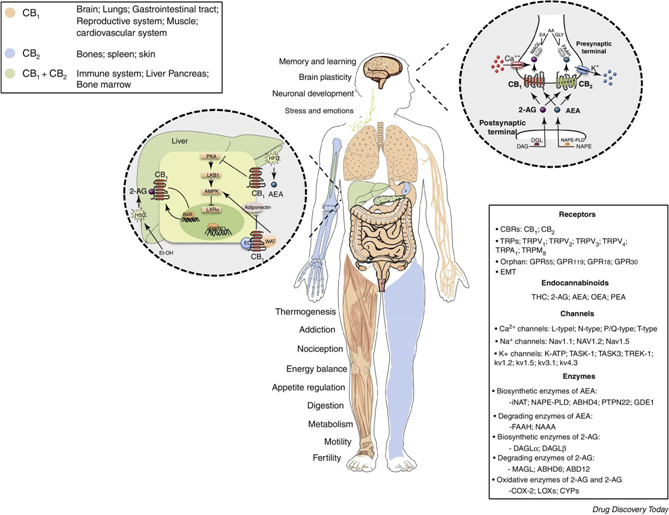
potent drug classified as a sedative-hypnotic. This was followed by the discovery of 2 cannabinoid receptors, CB1 and CB2, in the early 1990s.2 Both are G-protein-coupled receptors and serve as the primary site of action for THC. Together, they are involved in a major neuromodulatory system known as the endocannabinoid system (ECS). The primary goal of the ECS is to promote homeostasis.3 The main components of the ECS are the receptors CB1 and CB2; their endogenous ligands, ananda-mide (AEA) and 2-arachidonoylglycerol; and the enzymes that modulate their breakdown (fatty acid amide hydrolase and monoacylglycerol lipase). They are synthesized by fatty-acid metabolism and located in neurons, where they are released on demand by simple diffusion (Figure 1).4
The ECS is widespread
throughout the body, including the central and peripheral nervous systems. The
cannabinoid re-ceptors differ in their location of distribution. CB1 receptors
are found throughout the central nervous system and some periph-eral tissues.
CB2 receptors, on the other hand, are primarily found in peripheral tissues and
immune cells. Centrally, these receptors are more densely expressed in the
neurons of
Figure 1. The endocannabinoid system: its functions, distribution, and components. Figure 1 is available in color online.
| Effects of Cannabinoids on Female Sexual Function | 3 |
hypothalamus, hippocampus, amygdala, cerebral cortex, parts of the basal ganglia, and cerebellum. Peripherally, cannabinoid re-ceptors are found in organs responsible for producing sex hor-mones, such as the adrenals, which provide a source of androgens, and the ovaries, which provide a source of estrogen, progesterone, and androgens.5 Other biologically active canna-binoids (reviewed in Cohen et al6) have been discovered in marijuana, including cannabidiol, which is beginning to show promise in blocking pain and inflammation and for use as an antiepileptic medication; cannabigerol, which can treat the intraocular pressure associated with glaucoma; cannabichromene, which blocks pain and inflammation and shows encouraging anticancer effects; and tetrahydrocannabivarin, which acts as an effective appetite suppressant, reduces anxiety without altering mood, and shows efficacy in maintaining blood sugar levels and reducing insulin resistance. However, in addition to their inter-action with CB1 and CB2 receptors, these molecules modulate the binding affinity of other neurotransmitter receptors (eg, dopamine, serotonin). Importantly, the effects of these molecules have not yet been tested on sexual behavior.
ECS and the Hypothalamic Pituitary Axis
Studies have shown that a relationship exists between the ECS and gonadal hormones. The ECS has been implicated in certain physiologic functions and behaviors that are known to be regu-lated by gonadal hormones. Many of the receptors and metabolic enzymes of the ECS are located extensively in the structures involved in the hypothalamic-pituitary-gonadal axis. In animal models, studies show that THC suppresses gonadotropin release through the blockade of gonadotropin-releasing hormone from the hypothalamus.4 This in turn causes decreased luteinizing hormone and follicle-stimulating hormone release from the anterior pituitary, resulting in decreased estrogen release from the ovaries and decreased progesterone release from the corpus luteum.4 Thus, overall, THC blunts the activation of hormones that affect female sexual function.
Cannabinoids and the Neurotransmitters That Affect Sexual Function
CB1 is a presynaptic receptor that results in inhibition of neurotransmitter release when activated.7 CB1 receptors are located in the axon terminals of GABAergic, dopaminergic, adrenergic, glumatergic, and cholinergic neurons. Haring et al8 also found evidence of CB1 receptors in a subset of seroto-nergic neurons. Of importance, dopamine and serotonin play key roles in sexual functioning.9 Dopamine and norepinephrine play a role in excitatory processes of sexual function, such as desire and arousal, and serotonin plays a role in inhibitory pro-cesses, such as loss of desire. These neurotransmitters interact with testosterone, estrogen, melanocortins, progesterone, pro-lactin, and oxytocin to modulate the female sexual response.10
In the early 1970s, interest
grew in studying the effects of marijuana on sexual function. It was known that
marijuana had
effects on reproductive function. Marijuana was found to lower testosterone, decrease the weight of the testes, and affect sper-matogenesis in male rats.11 In female rats, marijuana was shown to decrease the luteinizing hormone surge and inhibit ovulation.12e14 It was therefore postulated that, due to its in-fluence on reproductive hormones, marijuana and other endo-cannabinoids might diminish sexual function. At that time, however, work on the effects of marijuana on sexual behaviors was limited; therefore, studies were done with animals, primarily rodents, to further elucidate the link between cannabinoids, including marijuana and sexual function.
Preclinical Studies of the Effects of Cannabinoids on Sexual Function
In 1978, Gordon et al11 evaluated the effects of THC on female lordosis, a posture assumed by some female mammals during mating, in which the back is arched downward. In rats, lordosis is a measure of female sexual receptivity. One goal of the study by Gordon et al was to determine if THC acted like es-trogen or progesterone. When these hormones were absent, these researchers found there was no effect on lordosis; however, when these hormones were present, THC enhanced lordosis, although at very high doses it did not.11
In 1981, Turley and Floody15 found that THC stimulated lordosis (receptivity) and sexual solicitation of a male (pro-ceptivity), along with precopulatory vocalizations, in ovariecto-mized, estrogen-primed hamsters. These results showed that the effects of THC could be extended to other species and other sexual behaviors. Mani et al16 found that THC infused into the third ventricle of the rat brain enhanced lordosis. This effect was blocked by the cannabinoid antagonists SR141716A and SR144528. The endocannabinoid antagonists were found to block progesterone-induced lordosis, also. Mani et al further evaluated receptivity when progesterone and dopamine were blocked and showed that receptivity was inhibited. These results imply that THC-induced receptivity is mediated by dopamine and progesterone.
Selective endocannabinoid receptor agonists and antagonists have also been examined with regard to sexual responses in fe-male rodents. Memos et al17 carried out a series of experiments evaluating the effects of the endocannabinoid antagonist SR141716 and the effects of the endocannabinoid agonist AEA on partner preference when compared with a placebo in rats. Sexual motivation was measured by the number of visits the female rats made to the male rats. They showed that AEA enhanced sexual motivation as measured by more visits from the female rats, and SR141716 inhibited it. They also found that AEA and SR141716 did not affect lordosis. Zavatti et al18 had somewhat different results, finding that SR141716 inhibited lordosis but not motivation in female rats.
Not all animal studies have yielded similar results. Ferrari et al19 evaluated the effects of a potent cannabinoid receptor agonist, HU-210, in female rats and found that administration.
| Sexual motivation | (runway test) | — | — | — | Decreased | Increased | — | Increased | Decreased | ||||
| Proceptivity(ultrasound vocalization | or hops and darts) | — | Increased | — | — | — | — | Increased | — | ||||
| Receptivity (lordosis) | Increased (low dose)Decreased(highdose) | ||||||||||||
| Increased | Increased | — | — | Decreased | Increased | — | |||||||
| Type of animal | Simonsen Sprague-Dawley rats | Golden hamsters | Sprague-Dawley rats | Long-Evans rats | Long-Evans rats | Wistar rats | Long-Evans rats | Long-Evans rats | |||||
| Table1.Summaryofpreclinicalstudies | Mechanism | of action | Agonist | Agonist | Agonist | Antagonist | Agonist | Agonist | Antagonist/reverseagonist | Agonist | ¼¼AEAanandamide;THCtetrahydrocannabinol. | ||
| AuthorDrug | Gordonetal(1978) | TurleyandFloody(1980) | Manietal(2000) | Memosetal(2014) | AEA | Ferrarietal(2000) | Lopezetal(2009) | Chadwicketal(2011) | |||||
| THC | THC | THC | SR141716 | HU-210 | AM-251 | CP 55,940 | |||||||
| 15 | |||||||||||||
| 11 | 16 | 17 | 19 | 20 | 22 | ||||||||
decreased both lordosis and the intensity of lordosis movements. The effect was dose and time dependent. Lopez et al20 evaluated receptivity, proceptivity, and sexual motivation as measured by a runway test. The runway test measures how fast a female rodent runs to a male rodent after being released from a chamber and is used as a surrogate for sexual motivation. They found that AM-251, an endocannabinoid antagonist/reverse agonist, enhanced these sexual behaviors. Lopez et al21 then evaluated a different cannabinoid receptor agonist, CP55,940, and found that sexual behaviors and motivation were decreased. Another study by Chadwick et al22 showed similar results with CP55,940. In rats, it decreased sexual motivation. Interestingly, female rats in this study showed no preference for a female or male mate when treated with CP55,940 but showed a male preference in the control group.
The varied findings in the animal studies likely reflect a series of factors. Different strains of animals, different types of agonist and antagonists, and different surrogate markers of sexual func-tion (proceptive vs receptive vs locomotor measures of motiva-tion) have been used. In addition, different compounds have different affinities for cannabinoid receptors. Routes of admin-istration are varied, as well (intracerebral vs systemic). Finally, the hormonal milieu in the animals varied among natural hormonal fluctuations, lack of hormones, or hormone replacement. Despite these limitations, animal studies provide some evidence that cannabinoids play a role in female sexual function, both directly and through interaction with the hypothalamic-pituitary-gonadal axis (Table 1).
Clinical Studies of the Effects of Cannabinoids on Female Sexual Function
Compared to the animal literature, there have been far more studies of the effect of marijuana on human female sexual function, although, to date, these findings have been limited to self-reported data. Despite the inability to conduct legal double-blind, randomized, placebo-controlled trials at this point in time in the United States, some data have been published to support the hypothesis that female sexual function is improved when women use marijuana in moderate doses.23e25 These studies are based on questionnaires, which are potentially fraught with bias.
Surveys of Males and Females Evaluating Effects of Marijuana Use on Sexual Function
In one of the earliest studies, the National Commission on Marihuana and Drugs23 reported findings from an informal survey of about 200 marijuana users who were asked, “Do you think being high on marijuana stimulates your sex interest, or not?” Among these 200 users, 44% reported “definitely increases their sexual desire, ” with 50% of those being women. They found that women were more likely than men to report an in-crease in desire. They also looked at rare, frequent, and heavy everyday marijuana use. Frequent but not daily marijuana use when compared to heavy everyday use and rare use (less than 1 joint a week) was associated with increased sexual pleasure in around 70% of users.
In 1974, Koff26 performed a survey of 251 college-aged stu-dents, who were asked about the amount of marijuana smoked each time the drug was used (1 joint or less, 2e4 joints, or more than 4 joints) and whether their sexual desire increased, decreased, or remained the same. He also asked whether sexual activity was more or less enjoyable after marijuana use. Of the 251 college students surveyed, 128 were female. The results of the survey indicated that 39.1% of males reported an increase in sexual desire, whereas 57.8% of females reported an increase—a significant difference (P ¼ .048). Also, 43% of the female participants re-ported heightened sexual pleasure. Additionally, Koff found that the effects of marijuana appeared to be dose dependent, noting that, although 71% of female participants reported increasing sexual motivation after 1 joint, the percentage of women reporting increased desire decreased after a larger consumption of marijuana (greater than 4 joints) (49.5%). This study supports the idea that the effect of marijuana on sexual function is dose dependent, such that low doses of marijuana (1 joint) can be sexually stimulating but high doses of marijuana can have the opposite effect.
In 1976, Chopra and Jandu27 interviewed 275 chronic marijuana users (smoked for 6 months to several years) from India and Nepal about the effects of marijuana and included some questions evaluating its effects on sexual function. This study observed similar dose-dependent effects and speculated that sexual inhibition is caused by an increased sedative effect seen at higher doses of marijuana intoxication. They did not divide their findings by gender.
A survey of 84 graduate students of health sciences in the southeastern United States was conducted by Dawley et al28 (78% male and 22% female). This survey included 57 multiple-choice and true/false questions that were developed to determine the attitudes of individuals regarding the effects of marijuana use on sexual function. The 84 graduate students were categorized as “experienced” (having had a sexual experience while under the influence of marijuana), “non-experienced” (those who have been under the influence of marijuana but have not concurrently had a sexual experience), and “non-smokers.” The study found that the “experienced participants” reported increased sexual pleasure (88%), sensations (48%), and satisfac-tion when both partners used marijuana (76%), as well as an increase in the intensity of the orgasm (58%). However, this study did not explore any differences between males and females, specifically.
These findings were further
replicated in a 1982 survey done by Halikas et al.29 One hundred regular marijuana users
(37 female users) with an average smoking experience of 2 years were
systematically interviewed to assess the psychosocial effects of marijuana use,
including effects on sexual function. This study demonstrated that 76% of
females reported an increase in sexual pleasure and satisfaction (14% of women
reported variable feelings), and 63% of women reported feelings of emotional
closeness and intimacy. Additionally, 32% of women reported an enhanced quality of orgasm, and the other 8% and 60% reported variable or no effects, respectively. Overall, 81% of people (men and women) reported pleasure-enhancing effects associated with marijuana use.
Data by Green et al30 support the previous finding by Halikas et al. Their review showed that approximately half of marijuana users reported increased aphrodisiac effects from marijuana use. Among regular marijuana users, 25% of them used marijuana in preparation for sexual intercourse. Of these users, over half re-ported increased sexual desire.
In 2004, Johnson et al31 conducted a survey-based, commu-nity epidemiological sample looking at the incidence and prev-alence of sexual dysfunction in the general population (inhibited orgasm, functional dyspareunia, inhibited sexual excitement, and inhibited sexual desire). Out of the 3,004 participants, 60% were female. After controlling for multiple variables such as de-mographics, health status, and psychiatric comorbidities, mari-juana was found to be associated with inhibited orgasm, as well as inhibited sexual excitement and desire. As opposed to the other studies mentioned in this review, Johnson et al asked survey questions specifically about sexual dysfunction, as opposed to general sexual function, and about comorbid drug and alcohol use. They did not ask questions about the potential benefits or experiences of marijuana usage, which perhaps played a role in why their results suggest a negative effect from marijuana.
Sumnall et al32 surveyed 281 sexually active volunteers regarding the effects of alcohol and drugs on their sexual be-haviors; 131 (48.5%) of the volunteers were female. The most commonly reported drug used was marijuana (46.9%), although some individuals reported mixing alcohol with drugs. Their study reported that both marijuana and ecstasy were more frequently taken to improve the sexual experience than alcohol. Those who had taken illicit drugs reported greater sexual plea-sure, increased mental/interpersonal contact with their sexual partner, greater willingness to sexually experiment, and a more satisfying sexual experience overall, indicating a greater total scale score for sex on drugs compared to alcohol (z ¼ 5.696; P <
.001). Although Sumnall et al found that it was not possible to distinguish the effects of different specific drugs, the overall effect was a more positive sexual experience on illicit drugs, including marijuana, compared to consuming alcohol.
In 2018, Palamar et al24 evaluated self-reported sexual
effects of marijuana, ecstasy, and alcohol use in a group of 679 men and women
(ages 18e25); 38.6% of the respondents
were women. When focusing on marijuana users, both male and female, the
majority reported increased sexual enjoyment (53.5%), orgasm intensity (44.9%),
sexual intensity (61.8%), body sensitivity (49.1%), and either an increase
(31.6%) or no change (51.6%) in sexual desire. Although this study did not
specifically analyze male
and female differences, the authors did note that females in their survey were
more likely than men to report sexual
dysfunction (30.6%), which was defined for survey takers as “vaginal dryness,” after marijuana usage. They also noted that this definition of sexual dysfunction was limited and that par-ticipants may have experienced other forms of sexual dysfunction.
Female-Only Surveys Evaluating the Effects of Marijuana Use on Sexual Function
Sun and Eisenberg33 surveyed 28,176 women via household laptops in 2002, 2006e2010, and 2011e2015. Women were asked, “Now please think about the past 4 weeks. How many times have you had sexual intercourse with a man in the past 4 weeks?” This was followed by, “During the past 12 months, how often have you smoked marijuana?” with the choice of responses being never, once or twice during a year, several times during the year, approximately once a month, approximately once a week, or at least once a day. They found that a higher frequency of marijuana usage was associated with increased sexual frequency. Although association does not imply causation and potential confounders existed in this study, including the exclusion of homosexual encounters and acknowledgment that those who use marijuana regularly might already be psychologically more dis-inhibited in general compared to those who do not use, the authors suggested that marijuana’s impact on and potential benefit for sexual function should be further studied.
25 conducted a survey of 373 women from 2016 to 2017 to evaluate women’s perceptions of the effect of marijuana usage before sexual activity. Of the 373 women, 127 reported using marijuana before sex. The majority of women reported increases in sex drive, improvement in orgasm, and a decrease in pain. Specifically, women who reported regular marijuana usage before sexual activity had 2.13 higher odds of reporting satis-factory orgasms. Women with frequent marijuana usage had 2.10 times higher odds of satisfactory orgasms than those with infrequent usage. observed that there appears to be a link between marijuana usage and satisfaction with orgasm, as well as with improvements in other domains of sexual function, a better understanding of which may lead to the development of treatments for female sexual dysfunction.
Serum Endocannabinoid Levels and Sexual Function
In 2012, Klein et al5 chose a more direct method of
studying the endocannabinoid system and its effects on female sexual function.
Their aim was to measure circulating endocannabinoid concen-trations in
relation to subjective and physiological indices of sexual arousal in women.
They measured physiological sexual arousal with vaginal photoplethysmography,
specifically measuring
vaginal pulse amplitude, which reflects
phasic changes in vaginal engorgement with each heartbeat. The overall concept
is that higher amplitudes indicate greater genital engorgement.
Endo-cannabinoid concentrations (AEA and 2-arachidonoylglycerol) in 21 healthy
premenopausal women were measured immediately
prior to and following viewing of both neutral and erotic films. Results indicated that increases in both physiological and subjec-tive measurements of sexual arousal were associated with signifi-cant decreases in levels of endocannabinoids. These findings support the hypothesis that the endocannabinoid system is involved in female sexual functioning and may well be inhibitory (Table 2).
DISCUSSION
Based on the above review of the literature, the most common sexual domains that have been evaluated include arousal, desire or “libido,” orgasm, pleasure, dyspareunia, vaginal lubrication, and duration of intercourse. Several studies have evaluated the effects of marijuana on libido, and it seems that changes in desire may be dose dependent. Studies support that lower doses
improve desire but higher doses either lower desire or do not affect desire at all.23,26,27
When evaluating sexual pleasure, most studies show that marijuana has a positive effect.27,30,31 Marijuana use with sex has
also been associated with prolonging orgasm or improving the quality of orgasm.5,24,34 Only 1 study that we reviewed reported
that marijuana use inhibits orgasm31; however, that study spe-cifically looked at dysfunction as opposed to overall function. Although our search revealed no articles that found an associa-tion between marijuana use and vaginal lubrication,35,36 this does not rule out such an effect, or an effect on vaginal blood flow, especially with a peripheral application.
Limitations
The body of evidence evaluating the effects of marijuana on female sexual function has several limitations. Although animal studies provide some information, there are no double-blind, randomized, placebo-controlled human trials from which to form a conclusion. The available human studies rely on recall and questionnaires. They are also quite different from each other. No validated questionnaires have been used, making it difficult to compare the results. Moreover, the specific wording of the ques-tions regarding libido, orgasm, pleasure, and pain all differed in both content and positive or negative valence. Some studies used questionnaires, and some used interviews. Some focused on marijuana users specifically, whereas others focused on a general population. Populations ranged from university students to pa-tients in an obstetrics and gynecology practice. Most studies focused on sexual function, but a single study evaluated potential sexual dysfunction. No human studies were able to evaluate the exact dose or timing of use. It is therefore difficult to make broad generalizations about the effects of marijuana on female sexual function based on available evidence.
It must be noted here that the other cannabinoids in mari-juana have not been tested empirically with regard to their effect on the sexual behavior of female rats or humans, although a recent study by Carvahlo et al37 reported an overall decrease
Table 2. Summary of clinical studies
| Author | Type of marijuana usage | Gender | Sexual desire | Sexual pleasure | Other findings | |
| US Commission on | Rare vs frequent vs heavy | Male and female (200 | Definite increase in sexual | — | Frequent, but not every | |
| Marihuana and | participants) | desire reported by | day, marijuana use | |||
| Drug Abuse (1972)23 | 44% (44, or 50%, of | (compared to usage | ||||
| whom were female) | every day) was | |||||
| associated with | ||||||
| increased sexual | ||||||
| pleasure in 70% of | ||||||
| users | ||||||
| Koff (1974)26 | One joint or less vs 2e4 | Male and female (251 | Increase in sexual desire | Heightened sexual | Effects of marijuana | |
| joints vs >4 joints | participants; 128 | noted by 57.8% of | pleasure reported by | appeared to be dose | ||
| females) | females | 43% of female | dependent; 71% of | |||
| participants | female participants | |||||
| reported increasing | ||||||
| sexual motivation | ||||||
| after 1 joint, but this | ||||||
| percentage decreased | ||||||
| after greater | ||||||
| consumption (>4 | ||||||
| joints) to 49.5% | ||||||
| Chopra and Jandu | Chronic cannabis users | Male and female (275 | — | — | Dose-dependent effects | |
| (1976)27 | (smoking 6 mo to several | participants) | with marijuana similar | |||
| years) | to the findings by Koff | |||||
| Dawley et al (1979)28 | Experienced (having had sex | Male and female (84 | — | Increased sexual pleasure | Increased sensations | |
| while under the influence | participants) | reported by 88% of | (48%) | |||
| of marijuana) | participants | Increased satisfaction | ||||
| vs non-experienced | with both partners | |||||
| (under the influence but | using (76%) | |||||
| no sexual experience) vs | Increase in the intensity | |||||
| non-smokers | of orgasm (58%) | |||||
| Halikas et al (1982)29 | Average smoking experience | Male and female (100 | — | Increase in sexual | 63% of women reported | |
| of 2 y | participants; 37 | pleasure and | emotional closeness | |||
| females) | satisfaction reported | and intimacy | ||||
| by 76% of females | ||||||
| Overall, 81% of | 32% of women reported | |||||
| participants reported | an enhanced quality of | |||||
| pleasure-enhancing | orgasm | |||||
| effects | ||||||
| Green et al (2003)30 | — | Male and female | Increased sexual desire | — | — | |
| participants | reported by w50% | |||||
| (continued) |
| Author | Type of marijuana usage | Gender | Sexual desire | Sexual pleasure | Other findings |
| Johnson et al (2004)31 | Marijuana usage and | Male and female (3,004 | Inhibited desire | — | Inhibited orgasm and |
| comorbid alcohol/drug | participants; 60% | sexual excitement | |||
| usage | female) | ||||
| Sumnall et al (2007)32 | Marijuana usage and | Male and female (131 | — | Increased sexual pleasure | Increased mental and |
| comorbid drug usage | participants; 48.5% | interpersonal contact | |||
| female) | with sexual partner | ||||
| Increased satisfaction | Greater willingness to | ||||
| with sexual experience | sexually experiment | ||||
| Klein et al (2012)5 | Measured circulating serum | — | — | — | Increases in both |
| endocannabinoid | physiological and | ||||
| concentrations | subjective | ||||
| measurements of | |||||
| arousal, which were | |||||
| associated with | |||||
| decreases in serum | |||||
| endocannabinoids | |||||
| Sun and Eisenberg | Never, once or twice a year, | Female | — | — | Higher frequency of |
| (2017)33 | several times a year, once | marijuana usage | |||
| a month, once a week, | associated with | ||||
| or at least once a day | increased sexual | ||||
| frequency | |||||
| Palamar et al (2018)24 | Marijuana, ecstasy, and | Male and female (679 | Increase or no change in | Increased sexual | 44.9% reported |
| alcohol | participants; 38.6% | sexual desire reported | enjoyment reported by | increased orgasm | |
| women) | by 31.6% | 53.5% | intensity | ||
| 30.6% of women | |||||
| reported sexual | |||||
| dysfunction (vaginal | |||||
| dryness) | |||||
| (2019)25 | Regular or frequent | Female | Increase in sex drive | — | 2.10 times higher odds of |
| marijuana usage | reported by majority of | satisfactory orgasm | |||
| women | with frequent | ||||
| marijuana usage; 2.13 | |||||
| times higher odds | |||||
| with regular marijuana | |||||
| usage |
fertility in female Swiss mice. It is also the case that the THC and cannabidiol content differs dramatically in different strains of marijuana,38 particularly in the marijuana that has been used legally in research, relative to strains consumed recreationally.39 This makes it impossible both quantitatively and qualitatively to compare the effects of laboratory-based intoxication with studies that examine retrospective experiences.
Clinical Implications
A better understanding of the
role of the endocannabinoid system in female sexual function has important
clinical impli-cations. Sexuality is complex, and the ECS is only one small
part of it. A clearer understanding may lead not only to the devel-opment of
therapeutic options for women but also to a deeper understanding of the
mechanisms involved in sexuality. With increasing legalization, there is the
potential to carry out more rigorous trials evaluating the exact dosing and
timing of use as opposed to using recall. This may lead to more substantive
conclusions than the animal and human studies have allowed us thus far.
Conflict of Interest: None.
Funding: None.
STATEMENT OF AUTHORSHIP
Category 1
Becky Lynn; Amy Gee; Luna Zhang
Becky Lynn; Amy Gee; Luna Zhang; James G. Pfaus
Becky Lynn; Amy Gee; Luna Zhang; James G. Pfaus
Category 2
Becky Lynn; Amy Gee; Luna Zhang; James G. Pfaus
Becky Lynn; Amy Gee; Luna Zhang; James G. Pfaus
Category 3
Becky Lynn; Amy
Gee; Luna Zhang; James G. Pfaus
CONCLUSION
Female sexuality is a complex interplay of environmental, psychological, and physiological processes. Multiple neurotrans-mitters and hormones play a role in sexual excitation and inhi-bition. The information we have is limited to rodent studies and questionnaires that rely on memory, with none of the human studies yet being capable of delineating dose, timing, or other objective measures. Although there appears to be a dose de-pendency that separates putative excitatory effects from inhibi-tory effects on female sexual desire, orgasm, and reproductive function, and frequency of use also plays a role, it is not clear to what extent the psychoactive properties of the various cannabi-noids play a role. For example, it is possible that the sedative hypnotic properties of THC and tetrahydrocannabivarin at low doses disinhibit sexual desire and arousal in response to erotic cues, but perhaps this occurs to a large extent in women who experience anxiety about sex or other interpersonal interactions. With recent decriminalization in México, and legalizations in Canada and certain US states, the Northern Hemisphere is now ripe to develop the high-quality, evidence-based studies necessary to answer important questions regarding marijuana and female sexuality. Like any drug, marijuana has risks and side effects and should be used with that in mind. A compre-hensive understanding of the effects of marijuana and its con-stituent cannabinoids on female sexual function remains to be elucidated.
Corresponding Author: Becky
Lynn, MD, Department of Obstetrics,
Gynecology and Women’s
Health, Division of General Obstetrics and Gynecology, Saint Louis University
School of Medicine, St. Mary’s
Hospital, 6420 Clayton Rd., St. Louis, MO 63117; E-mail: [email protected]
REFERENCES
hypoactive sexual desire disorder and treatment options.
10
estrogen treated female rats. Pharmacol Biochem Behav 1978; 8:603-608.
related to alcohol and marijuana use among adults. Arch Sex Behav 2018;47:757-770.
Source: PDF
Allowing chemotherapy drugs directly into the cancer cells without harming healthy cells is the latest word in cancer research - there are chemotherapy drugs that are not stylized to penetrate the cancer cell program. Combining the chemotherapeutic drug with cannabidiol (CBD) to infiltrate the cancer cell and kill it from within - according to a new Israeli study conducted at the Hebrew University.
Shay Friedman
A new study from the Hebrew University published last month in the Pharmacology Frontier Journal found that chemotherapy with cannabidiol (CBD), the national ingredient for mastyl agri in the cannabis plant, should be believed that other entities while the movies were improving its efficacy and reducing its side effects.
Trials have developed a new method for injecting chemotherapeutic drugs directly into cancer cells, through such small channels as "TRP channels". In their previous studies, they have already been able to inject several different types of drugs directly into the malignant cells by this method.
The commander of the new method is significant - targeting the drug exclusively in cancer cells prevents it from damaging the healthy homes that are massive, as if significantly exposing the side-effects of the relationship and enhancing its services.
The researchers tried to use them as a method to introduce the chemotherapeutic drug doxorubicin (doxorobicin) into liver cancer cells and actually kill them from the inside. Doxorubicin is a very effective drug for the core in various cancers, but it also damages healthy homes in the body and causes serious side effects, can be a cause of heart failure.
The researchers hypothesized that the drug doxorubicin directly into the cancer cells. The way to increase TRP using the method they developed would significantly reduce the histopathological side effects and increase its units. But docsorubicin is very difficult to penetrate a way to increase TRP, and this is where the CBD comes into play.
CBD improves chemotherapy penetration into cancer cells
The researchers found that CBD has the ability to activate the TRPV2 name protein, and its elevation opens access to the TRP in the liver cancer cells, and the doxorubicin can be introduced. In other words - CBD can be injected directly into the cancer cells and only to them can get the damage to the healthy homes around.
CBD is not the only material that Google has unlocked to raise the TRP - in the past it was already discovering a substance called 2-APB that does just that. In the present study, the researchers compared the role of docorubicin in combination with CBD, as well as in combination with 2-APB, and found that administering a drug with CBD is much more effective, requiring significant doses of necrosis.
"We have shown that a combination of CBD or 2-APB that triggers TRP elevation, together with dororubicin, results in america concentrations of the dorsorbucin within cancer cells that put the resources into repressing the single dororubicin," the study notes.
"In addition, we have shown that low doses of doxorubicin in combination with 2-APB or CBD result in a significant decrease. Liver cancer cells live and their colonies compared to doxorubicin alone. Finally, we have also shown that combining doxorubicin with CBD kills far more liver cancer cells and their colonies. Compared to the combination of doverorubicin with 2-APB.
The study was led by my colleague, Professor Alexander Beinstock
"Since the test used a chemotherapy component that is already equipped with clinical use, responsible for integrating the concept office into laboratory animals, moving to the next phase of a human trial that could be shorter," Professor Hinstock said when asked how long it would take to use the new method on the patient. cancer. "It's still too early to predict, but we're hopeful we have what a reactor can do at the end of the tunnel."
Source: https://www.frontiersin.org/articles/10.3389/fphar.2019.01198/full

TOGETHER - PANAXIA - BAZELET
In order to be able to recognize the goods in Israel, the company must adhere to two rules: the GAP growth standard is the production count and the laboratory tests in Israel.
Will the Cannabis Medical Company be able to get the Health Ministry official to import her crops from Uganda? The undertaker's office did not disclose to the German scholarship the material it had grown in Uganda, at least until it obtained a relevant permit to prepare the goods from the German regulator.
Together (+ 3.76% 386.8), managed by Nissim Bracha, explained to the Games in Israel that she is planning a first commercial harvest of 5,000 medical cannabis seedlings on a farm in Uganda, inspired by 30 acres. This modern society was not intentional, it is aware that the law in Israel is not the establishment of medical cannabis direct sales to patients.
The Marker learned that three additional requests for import were placed on the Ministry of Health table and were pending no contact: Panaxia, its Lod plant; Bazalet Company, which holds the largest waterfall in Israel; Private led by Attorney Sagi Beno, who applied for approval to import goods into Israel.
Sales of 60,000 patients in Israel, and the new reform that led to the third books are three on cannabis products.
In order to be able to recognize goods in Israel, the importing company must adhere to two main rules: the GAP standard of production growth and laboratory tests in Israel. Proper home file size of water and air, the lab will check for pesticides in the plant. This check makes the Department of Health ascertain the quality of the water that fed the plant - an issue that may plague quite a few patients who fear water in Uganda may endanger the bars.
In practice, it seems that it will be much more difficult to convince the Ministry of Health that they comply with the Israeli or European regulation. The effort it takes to import cannabis from Uganda to Israel will be greater than that of its companies importing Europe-size material under EU rules.
Uganda does not have a mutual recognition agreement with Israel, so the Ministry of Health and the Ministry of Agriculture will need to ensure that Togder grows the goods under the right conditions. Such an examination would require a party from the Ministry of Health or another body in its authority to travel to Uganda and inspect the goods before bringing them to Israel.
Nir Sosinski, the controlling shareholder, in Together: "There are two options for the material broadcaster coming from Uganda. The truth comes from the model of Israeli farms. A half-pound biopsy for a GMP approved waterfall, packed in 10 grams and trays for the final consumer. The second option is that the Ministry of Health knows the books GMP Existing and Services from Ugandan Ministry of Health I know this for the country.
"World Union Control, which also works with the ministry in Israel, has arrived in Uganda, and the support for access to GACP development. The reports on this in the past. To get to know the bunch to the country we can show the cheerleaders the relevance and testing of the lab and then import. The European standard we work on in Uganda We check the permissible air before and after flowering, we have certificates on every part of the process.
Source: https://www.themarker.com/markets/1.8160111
A rumor of rumors from the corridors of the Ministry of Health and conference rooms is released like white smoke. News of documents that are already ready for signature and final approval, details of standards and procedures that will allow importers to engage in the field of Israel, and a lot of hopeful concern - when will that happen?
We in the Israeli CBD community are not concerned with prophecy and guesswork, but we strive to lead information and education to proper and smart consumption, developing education and information in an area that is unparalleled and important to everyone's health and well-being.
Over the past year and a half, we have worked with thousands of consumers on finding the right products and doses for a huge variety of medical and non-medical needs.
A combination of theoretical knowledge acquired daily by the experts in the field, together with experience in the field itself, brings us in line with what is happening in the world.
good week
The Israeli CBD community
Source: https://www.facebook.com/229470837773023/posts/447970135923091/
Drama in the industry: From now on, importation of medical cannabis from abroad is permitted even under stringent quality standards without the strict quality standards. The goal: to alleviate the shortage of pharmacies. The new Israeli cannabis farms may be damaged.
First publication: The Ministry of Health permits for the first time import of medical cannabis containing THC from abroad even without complying with the strict Israeli standard (IMC-GMP) or its corresponding standards, as well as in the form of raw material and not only as a finished product as permitted to date.
This decision by the Ministry of Health is a significant relief compared to the previous procedure that was also revealed in Cannabis magazine about five months ago and will only allow imports from companies that have the strict EU-GMP standard as well as only a finished and packaged product.
This is a big news for importers and patients, but in what is likely to provoke the anger of new cannabis farm owners in Israel that have been established and will rise to stringent standards in which tens of millions of NIS have been invested. Some have dreamed of receiving a price of NIS 5 and up per gram - which will probably not be possible now.
For example, an Israeli cannabis factory is now authorized to import tons of medical cannabis from farms that hold a basic GAP standard (e.g. Global GAP, as the farms held in the old series) and not just the stringent standard, as long as the raw material meets the cleanliness tests conducted in Israel.
Products that do not contain THC but only CBD can now be imported even without GAP or GMP standards at all, as long as they hold the approval of a dietary supplement. Once imported, they will have to pass through the Israeli production chain according to the procedures and for licensed patients only.
After the establishment of the government and the planned CBD exemption under the Drugs Ordinance, subject to the approval of the Health Commission, CBD and its products can be imported without passage through the production chain but directly to retailers and consumers without a medical cannabis license.
Cannabis Magazine's review also reveals that customs authorities have completed the procedures for importing previously unregistered cannabis, including "bonded" (warehouse) procedures for receiving the goods, and more.
On the one hand, some claim that there are not many productive countries that comply with the above procedures and that the products are usually more expensive than in the country and will therefore be complex and unprofitable to import such goods. On the other hand, some claim that medical cannabis can now be imported at very low costs - even up to 10 cents a gram.
Recall, as revealed in Cannabis Magazine, the Department of Agriculture objected to importing cannabis from abroad and even stated that the import approved by the Ministry of Health for Saiki was illegal. A review of Cannabis Magazine revealed that the Department of Health coordinated with the Department of Agriculture the new procedures to make this possible.
This update joins other eases reported by the Ministry of Health in its response to the High Court, as revealed in a magazine yesterday. Among other things, the number of quality tests will only be reduced to 1 at the end of the production process, new farms will be able to grow thousands of seedlings immediately instead of only 180, and more.
Regarding self-tumor permitting for medical cannabis patients, there was some regression. Despite the Secretary-General's statement that he does not rule out allowing this possibility, the Ministry of Health replied to a petition filed against it because it opposes it because it is contrary to the UN Drug Convention and that their position does not have a medical advantage.
Source: https://www.xn--4dbcyzi5a.com/%D7%9E%D7%A9%D7%A8%D7%93-%D7%94%D7%91%D7%A8%D7%99%D7%90%D7%95%D7%AA-%D7%9E%D7%AA%D7%99%D7%A8-%D7%99%D7%99%D7%91%D7%95%D7%90-%D7%A7%D7%A0%D7%90%D7%91%D7%99%D7%A1-%D7%A8%D7%A4%D7%95%D7%90%D7%99-%D7%95-c/

Ministry of Health plans to publish guidelines on cannabis export this Monday
• In a statement to the High Court, the Ministry said: "For the Ministry of Health, any business that meets the standard for local production and marketing - can market its products abroad"
• Exposure of regulations by the Ministry of Health still does not mean that Agreeing with all the parties involved in the matter and all barriers to export were removed, but at the very least it indicates that the discussion is progressing and not stuck
The Ministry of Health revealed in a reply to the High Court of Cannabis patients that the export of cannabis is approaching and that guidelines on the matter will be issued this Monday.
The decision to allow cannabis exports from Israel was made by the government in January, but so far it has not been clear when it will be implemented.
The Ministry of Health said: "For the Ministry of Health, any business that meets the standard for local production and marketing can also market the products abroad. In order to approve a specific batch, the Ministry will face inventory, variety, price and local availability, and no export will be possible. Proper supply of patients in the State of Israel will not be guaranteed. "
The document further states that "insofar as the Honorable Court does not otherwise order, the Ministry of Health intends to act to publish these regulations this Monday, November 18".
The document further states: "Insofar as it is found that any of the dealers do not fulfill the terms of their license, including the obligation to transfer cannabis or its products, as applicable, to the next link in the supply chain in quantity and at an appropriate price, the Ministry of Health will use all the tools at its disposal, including the revocation of the license. Or its limitation. "
The High Court of Cannabis was tabled by the Dana Brown Patient Association, claiming that cannabis reform disadvantages patients by making it more difficult to access products they have become accustomed to, and that has led to a steep rise in prices. The High Court has demanded from the Ministry of Health and Hickar, the medical cannabis unit in the office , Explain how to take care of the variety of products and prices.
Hanging the export with a proper supply of products to the domestic market, which has already hinted at in the past, is part of the firm's response to patient claims, but the wording of things and the statement that an orderly announcement will come out on Monday suggest that the time is coming to a close.
Cannabis companies in Israel have about 20 public companies and dozens of private companies. They compete in the country for only a few hundred million shekels a year. The value of the companies is in most cases derived from the export plans, and many of them also depend on exports to finance investments, which will enable them to operate competitively in Israel. Therefore, turning the export from a government decision into regulations allowing the actual launch is one of the dramatic events for this industry.
According to Attorney Hagit Weinstock of the Weinstock Zahavi office, one of the leading cannabis offices in Israel and especially in the interface between the country and abroad: "I believe that this is not a spin but a significant move in the right direction. "And then we got messages from the various government offices that we should wait a bit because something is going to happen."
Attorney Weinstock added, "In the past six foreign companies that I represent have announced their intention to reach an urgent country. I don't know how it came to them. For the past two weeks we have been witnessing something happening. Foreign investors who froze deals began to find out if the process could be started again. Meanwhile, the local market was also starting to move. For example, our client is a Togder company that has signed an agreement for tens of millions of shekels. We believe the local market will include 700,000 people. "
Weinstock also said that now the possibility of exporting to Germany, the main target country to which the eyes of the Israeli cannabis industry are referred, will also depend on German regulations. These require a very specific composition of the exported compound, which controls the level of many substances in the plant, and not only the two substances THC and CBD. Also, German regulation prefers enclosed greenhouses (indoors). In addition, only one cannabis plant, that of Panaxia, has been granted compliance with the proper conditions of production of the European Union, and it must be ascertained that this approval does also comply with the specific rules in Germany. Weinstock Zahavi said that she was accompanied by transactions of exports from other European countries to Germany, and the materials did not always meet the conditions. However, she notes, Germany's demand for products is large and the shortage is severe in Israel.
Source: https://www.globes.co.il/news/article.aspx?did=1001307403

A customer pays cash for retail marijuana at 3D Cannabis Center in Denver. The U.S House on Wednesday passed a bill that would protect banks that service cannabis businesses.
A MEASURE TO PROTECT financial institutions that service cannabis companies passed the House in a bipartisan vote Wednesday, becoming the first standalone marijuana reform bill to ever clear a chamber of Congress.
The legislation, if ultimately made into law, would protect financial institutions and ancillary firms that serve marijuana businesses from criminal prosecution and other consequences – a long-awaited move that would provide stability and security to the multi billion-dollar cannabis industry.
The measure, the Secure and Fair Enforcement Banking Act of 2019, passed the chamber by a vote of 321-103. Nearly all Democrats backed the bill as did 91 Republicans. It required a two-thirds majority to pass because it was voted on under a procedure that suspends House rules – a move that allows bills that enjoy broad but not unanimous support to be voted on quickly.
Eleven states and the District of Columbia have legalized the recreational use of marijuana, and a majority of states also have legal medical marijuana programs. But the drug remains illegal at the federal level, making banks and credit unions wary of doing business with the industry because of the threat of criminal prosecution and regulatory consequences. The SAFE Banking Act shields financial institutions who work with state and tribe-legal cannabis businesses from those consequences.
The bill moved out of the House Financial Committee in March and was sponsored by more than 200 lawmakers at the time of the vote. It is backed by a slew of national banking groups, including the American Bankers Association, the Credit Union National Association and the Independent Community Bankers of America, which have pushed Congress to act on the issue for some time. The National Association for State Treasurers, a bipartisan group of more than 30 state attorneys general, and the governors of 20 states have urged Congress to pass the bill.

Cannabis trade groups, marijuana legalization advocates and human rights groups generally support the measure, though some rights groups voiced concern that the banking bill would get in the way of broader reforms and federal legalization.
"We applaud the House for approving this bipartisan solution to the cannabis banking problem, and we hope the Senate will move quickly to do the same," said Neal Levine, chief executive officer of the Cannabis Trade Federation, which lobbied in support of the bill. "This vital legislation will have an immediate and positive impact, not only on the state-legal cannabis industry, but also on the many communities across the nation that have opted to embrace the regulation of cannabis. Allowing lawful cannabis companies to access commercial banking services and end their reliance on cash will greatly improve public safety, increase transparency, and promote regulatory compliance."
It's not clear what the measure's chances are in the Senate. The Senate version of the legislation is sponsored by 33 senators but hasn't yet made it out of committee. Sen. Mike Crapo, Idaho Republican and chairman of the Senate Banking Committee, told Politico he plans to mark up a cannabis banking measure in his committee before the year ends, though it may not be the banking bill that has already been introduced. It's not known if Senate Majority Leader Mitch McConnell of Kentucky would bring such a measure to a vote in the chamber.